[ad_1]
Positive reverse transcription polymerase chain reaction (RT-PCR) tests have been used as the justification for keeping large portions of the world locked down for the past nine months. Not reliable hospitalization or death rates; just positive PCR test numbers — a large portion of which are from people who have no symptoms of actual illness — are the triggers behind the shutdowns.
Experts are now coming forward in growing numbers denouncing mass PCR testing as foolhardy and nonsensical if not outright criminal. Why? Because we’re now finding that PCR tests rarely tell us anything truly useful, at least not when they’re used as they have been so far.
Why PCR Tests Are the Wrong Tool to Assess Pandemic Threat
We now know that PCR tests:
1. Cannot distinguish between “live” viruses and inactive (noninfectious) viral particles and therefore cannot be used as a diagnostic tool — For this reason, it is grossly misleading to refer to a positive test as a “COVID-19 case.”
As explained by Dr. Lee Merritt in her August 2020 Doctors for Disaster Preparedness1 lecture, featured in “How Medical Technocracy Made the Plandemic Possible,” media and public health officials appear to have purposefully conflated “cases” or positive tests with the actual illness.
Medically speaking, a “case” refers to a sick person. It never ever referred to someone who had no symptoms of illness. Now all of a sudden, this well-established medical term, “case,” has been arbitrarily redefined to mean someone who tested positive for the presence of noninfectious viral RNA. As noted by Merritt, “That is not epidemiology. That’s fraud.”
2. Cannot confirm that 2019-nCoV is the causative agent for clinical symptoms as the test cannot rule out diseases caused by other bacterial or viral pathogens.
3. Have not been established for monitoring the treatment of 2019-nCoV infection.
4. Have exceptionally high false result rates — The higher the cycle threshold (CT) — i.e., the number of amplification cycles used to detect RNA particles — the greater the chance of a false positive.
While any CT over 35 is deemed scientifically unjustifiable,2,3,4 the U.S. Food and Drug Administration and the U.S. Centers for Disease Control and Prevention recommend running PCR tests at a CT of 40.5
Drosten tests and tests recommended by the World Health Organization are set to a CT of 45. These excessively high CTs guarantee the appearance of widespread (pandemic) infection when infection rates are in fact low.
The CT Is the Key to the Pandemic
Many if not most laboratories amplify the RNA collected far too many times, which results in healthy people testing “positive” for SARS-CoV-2 infection and being ordered to take off work and self-isolate for two weeks.
To optimize accuracy and avoid imposing unnecessary hardship on healthy people, PCR tests must be run at far fewer cycles than the 40 to 45 CTs currently recommended.
An April 2020 study6 in the European Journal of Clinical Microbiology & Infectious Diseases showed that to get 100% confirmed real positives, the PCR test must be run at 17 cycles. Above 17 cycles, accuracy drops dramatically.
By the time you get to 33 cycles, the accuracy rate is a mere 20%, meaning 80% are false positives. Beyond 34 cycles, your chance of a positive PCR test being a true positive shrinks to zero, as illustrated in the following graph from that study.7
By running PCR tests at 40 to 45 amplification cycles, you end up with the false appearance of an outbreak, and this grossly flawed testing scheme is what government leaders are basing their mask mandates and lockdown orders on.
Percentage of positive viral culture of SARS-CoV-2 PCR-positive nasopharyngeal samples from Covid-19 patients, according to Ct value (plain line). The dashed curve indicates the polynomial regression curve.
Scientific Review Confirms PCR Flaws
More recently, a December 3, 2020, systematic review8 published in the journal of Clinical Infectious Diseases assessed the findings of 29 different studies — all of which were published in 2020 — comparing evidence of SARS-CoV-2 infection with the CTs used in testing. They also looked at the timing of the test, and how symptom severity relates to PCR test results. As reported by the authors:
“The data suggest a relationship between the time from onset of symptom to the timing of the specimen test, cycle threshold (CT) and symptom severity. Twelve studies reported that CT values were significantly lower and log copies higher in specimens producing live virus culture.
Two studies reported the odds of live virus culture reduced by approximately 33% for every one unit increase in CT. Six of eight studies reported detectable RNA for longer than 14 days but infectious potential declined after day 8 even among cases with ongoing high viral loads …”
In other words, if you have symptoms of COVID-19, by Day 8 from the onset of symptoms, the chances of you spreading it to others starts to decline, and in the days following, you are unlikely to be infectious even if you still test positive. This is particularly true if the PCR test is using a higher than ideal CT. As noted by the authors:9
“Complete live viruses are necessary for transmission, not the fragments identified by PCR. Prospective routine testing of reference and culture specimens and their relationship to symptoms, signs and patient co-factors should be used to define the reliability of PCR for assessing infectious potential. Those with high cycle threshold are unlikely to have infectious potential.”
Live Virus Unlikely in Tests Using CT Above 24
According to The New York Times,10 researchers have been “unable to grow the coronavirus out of samples from volunteers whose PCR tests had CT values above 27,” and if the virus cannot replicate, you will not get ill and are not infectious, so you cannot spread it to others.
The Clinical Infectious Diseases review11 confirms this. Under the heading “The Relationship Between RT-PCR Results and Viral Culture of SARS-CoV-2,”12 they point out that “significantly lower” CTs were used in studies that correctly identified infectious patients.
Five of the studies included were unable to identify any live viruses in cases where a positive PCR test had used a CT above 24. What’s more, in order to produce live virus culture, a patient whose PCR test used a CT at or above 35 had to be symptomatic.
So, to clarify, if you have symptoms of COVID-19 and test positive using a PCR test that was run at 35 amplification cycles or higher, then you are likely to be infected and infectious.
However, if you do not have symptoms, yet test positive using a PCR test run at 35 CTs or higher, then it is likely a false positive and you pose no risk to others as you’re unlikely to carry any live virus. In fact, provided you’re asymptomatic, you’re unlikely to be infectious even if you test positive with a test run at 24 CTs or higher.
Timing of PCR Test Also Matters
The Clinical Infectious Diseases review also confirmed that the timing of the test matters. According to the authors:13
“… there appears to be a time window during which RNA detection is at its highest with low cycle threshold and higher possibility of culturing a live virus, with viral load and probability of growing live virus of SARS-CoV2 …
We propose that further work should be done on this with the aim of constructing an algorithm for integrating the results of PCR with other variables, to increase the effectiveness of detecting infectious patients.”
Another scientific review14,15 that looked into how the timing of the test influences results and your risk of being infectious was posted on the preprint server medRxiv September 29, 2020. Fourteen studies were included in this review.
The data show that your chances of getting a true positive on the first day of COVID-19 symptom onset is only about 40%. Not until Day 3 from symptom onset do you have an 80% chance of getting an accurate PCR result.
By Day 5 the accuracy shrinks considerably and by Day 8 the accuracy is nil. Now, these are symptomatic people. When you’re asymptomatic, your odds of a positive PCR test being accurate is virtually nonexistent.
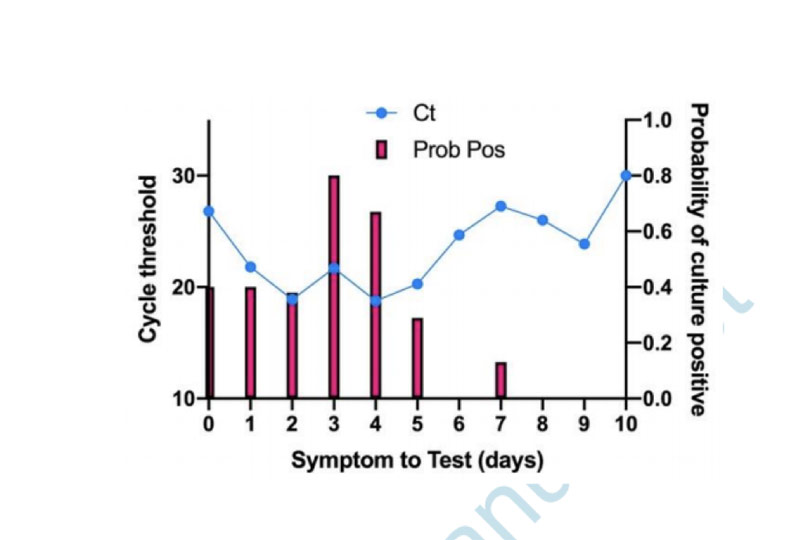
The graph below, from one of the studies16 included in the review (Bullard et. al.), illustrates the probability of a patient being infectious (having live virus) based on the CT used and the timing of the test. As explained by the review authors:17
“The figure … shows how the probability of SARS-CoV-2 infectious virus is greater (the red bars) when the cycle threshold is lower (the blue line) and when symptoms to test time is shorter — beyond 8 days, no live virus was detected.”
Florida to Require Disclosure of CT Data
Even though health authorities know that high CTs result in high rates of false positives, they do not specify the CT used for the PCR tests they’re reporting. Fortunately, that’s about to change in Florida, which just became the first state to require all labs in the state to report the CT used for their PCR tests.18
The Florida Health Department issued the order December 3, 2020, and labs must comply with the new mandatory reporting rule within seven days.19
This could prove quite interesting, especially if the state health department decides to invalidate positive results obtained from tests run above a certain amplification threshold. Time will tell exactly how this reporting requirement might influence pandemic response measures such as mask mandates and lockdowns.
Portugal Rules Quarantine Based on PCR Results Is Unlawful
In related news, an appeals court in Portugal recently ruled20,21 that the PCR test is “not a reliable test for SARS-CoV-2” and that “a single positive PCR test cannot be used as an effective diagnosis of infection.” Therefore, “any enforced quarantine based on the results is unlawful.”22
The court also noted that forcing healthy people to self-isolate could be a violation of their fundamental right to liberty. The case was brought by four German tourists who had been forced to self-quarantine after one of them tested positive.
Several scientific studies were brought forth as evidence in this case, including a September 28, 2020, study23 in Clinical Infectious Diseases, which found that when you run a PCR test at a CT of 35 or higher, the accuracy drops to 3%, resulting in a 97% false positive rate. The court ruled that, based on the science presented, any PCR test using a CT over 25 is unreliable.
Fatal Errors Found in Paper on Which PCR Testing Is Based
The Portuguese appeals court is not alone in its critique of the PCR test being used as the sole criteria for quarantine. November 30, 2020, the scientific paper24 describing the work flow of how to use the PCR test to diagnose SARS-CoV-2 infection — which was quickly accepted as the standard by the WHO and applied across the world — was challenged25 by 22 international scientists who demand that the paper be retracted due to “fatal errors.”26
The paper in question was written by Christian Drosten, Ph.D., a German virologist, and Victor Corman, who heads a German working group on virus diagnostics and clinical virology. According to Reiner Fuellmich,27 founding member of the German Corona Extra-Parliamentary Inquiry Committee (Außerparlamentarischer Corona Untersuchungsausschuss,28 or ACU),29,30 Drosten is a key culprit in the COVID-19 pandemic hoax.
One of the key “fatal errors” in the Corman-Drosten paper is that they wrote it — and developed the PCR test — before there was any viral isolate available. All they used was the genetic sequence published online by Chinese scientists in January 2020.
Interestingly, the paper was published a mere 24 hours after it was submitted, which suggests it wasn’t even peer-reviewed before being embraced by the whole world. Undercover DC interviewed Kevin Corbett, Ph.D., one of the 22 scientists who are now demanding the paper’s retraction, who stated:31
“Every scientific rationale for the development of that test has been totally destroyed by this paper. It’s like Hiroshima/Nagasaki to the COVID test.
When Drosten developed the test, China hadn’t given them a viral isolate. They developed the test from a sequence in a gene bank. Do you see? China gave them a genetic sequence with no corresponding viral isolate. They had a code, but no body for the code. No viral morphology.
In the fish market, it’s like giving you a few bones and saying ‘that’s your fish.’ It could be any fish … Listen, the Corman-Drosten paper, there’s nothing from a patient in it. It’s all from gene banks. And the bits of the virus sequence that weren’t there they made up.
They synthetically created them to fill in the blanks. That’s what genetics is; it’s a code. So, its ABBBCCDDD and you’re missing some, what you think is EEE, so you put it in … This is basically a computer virus.
There are 10 fatal errors in this Drosten test paper … But here is the bottom line: There was no viral isolate to validate what they were doing. The PCR products of the amplification didn’t correspond to any viral isolate at that time. I call it ‘donut ring science.’ There is nothing at the center of it. It’s all about code, genetics, nothing to do with reality …
There have since been papers saying they’ve produced viral isolates. But there are no controls for them. The CDC produced a paper in July … where they said: ‘Here’s the viral isolate.’ Do you know what they did? They swabbed one person. One person, who’d been to China and had cold symptoms. One person. And they assumed he had [COVID-19] to begin with. So, it’s all full of holes, the whole thing.”
No Viable Virus Found in Positive Cases
The critique against PCR testing is further strengthened by a November 20, 2020, study32 in Nature Communications, which found no viable virus in PCR-positive cases. The study evaluated data from 9,865,404 residents of Wuhan, China, who had undergone PCR testing between May 14 and June 1, 2020.
A total of 300 tested positive but had no symptoms. Of the 34,424 people with a history of COVID-19, 107 tested positive a second time. Yet when they did virus cultures on these 407 individuals who had tested positive (either for the first or second time), no live virus was found.
Expose the Fraud, End the Misery
A number of experts have now come forward, calling out the COVID-19 pandemic as a cruel hoax perpetuated by fatally flawed testing. Aside from this testing data, there’s no evidence of a lethal pandemic at all. While there is such a thing as COVID-19, and people have and do die from it, there are no excess deaths due to it.33,34,35
In other words, the total mortality for 2020 is normal. The pandemic has not killed more people than would die in any given year — from something, anything — anyway. So, unless we think we should shut down the world and stop living because people die from heart disease, diabetes, cancer, the flu or anything else, then there’s no reason to shut down the world because some people happen to die from COVID-19.
The good news is the hoax is starting to be exposed, and will continue to be exposed as more cases are brought before the courts of the world. Fuellmich and his ACU legal team are leading that charge. As for what you can do in the meantime, consider:
• Turning off mainstream media news and turning to independent experts — Do the research. Read through the science.
• Continue to counter the censorship by asking questions — The more questions are asked, the more answers will come to light. Arm yourself with mortality statistics and the facts on PCR testing, so you can explain how and why this pandemic simply isn’t a pandemic anymore.
• If you are a medical professional, especially if you’re a member of a professional society, write an open letter to your government, urging them to speak to and heed recommendations from independent experts.
• Sign The Great Barrington Declaration,36 which calls for an end to lockdowns.
• Join a group so that you can have support. Examples of groups formed to fight against government overreach include:
◦ Us for Them, a group campaigning for reopening schools and protecting children’s rights in the U.K.
◦ The COVID Recovery Group (CRG), founded by 50 conservative British MPs to fight lockdown restrictions37
◦ The Freedom to Breathe Agency, a U.S. team of attorneys, doctors, business owners and parents who are fighting to protect freedom and liberty
[ad_2]


{kind=link}